
Efficient planning - intuitive transfer to surgery
EyeSuite IOL offers latest generation IOL calculations such as the Hill-RBF Method, Barrett and Olsen for standard IOL, enabling improved results with any patient. It further includes a comprehensive set of premium post-refractive formulae, including Barret’s True-K and the Masket formula which are regarded as best in class. For torics it optionally offers a complete planning suite to calculate the implant, considering the front and back of the cornea and create intuitive surgery sketches, enabling excellent transfer of the plan to surgery.

Stay on target any time
Standard IOL calculations provide good results in average eyes; they fail in short and long eyes as well as eyes with special anatomic features. EyeSuite IOL features the Barrett and Olsen formula, enabling excellent refractive results with any patient anatomy.
Hill-RBF Method - Pursuing a new level of accuracy


Hill-RBF Method - Thinking out of the box for a new level of performance
Hill-RBF Method - Thinking out of the box for a new level of performance
For retrospective testing, looking at 3,212 independent cases from 13 surgeons in eight countries, the outcomes have been impressive with a weighted mean ±0.50 D accuracy of 95%.
“No one’s ever seen numbers like this,” Dr. Hill said.
What is even more impressive than the accuracy is the consistency from one beta test site to the next across Europe, the Middle East, Africa, North and South America, Asia, India, and Australia. This level of consistency reveals that the outcomes are technologically driven.
“In summary, this is a new approach based on pattern-recognition, data interpolation, and a validating boundary model, but just adds an additional level of confidence, and the accuracy of this methodology is due to an increase in flexibility,”
The RBF Method is now available on-line at: www.RBFCalculator.com and is going to be integrated exclusively in the Lenstar with the fall release of EyeSuite this year.


Lens thickness - improved results
Lens thickness - improved results
Barrett and Olsen use more directly related parameters to calculate the implant position. The most important parameters in this respect are anterior chamber depth (ACD) and lens thickness (LT). Modern IOLs are implanted in the capsular bag of the crystalline lens and therefore ACD and LT are directly related to the implant position post-operatively.


Barrett Universal II - a formula for all seasons
Barrett Universal II - a formula for all seasons


Olsen - the C-constant a new concept
Olsen - the C-constant a new concept
In a clinical series on more than 1700 eyes, Dr. Olsen assessed the performance of the Olsen formula as compared to standard formulae like Holladay 1 and SRK/T. All measurements were taken with Lenstar and independently of the eye length, the Olsen formula using the concept of the C-constant and paraxial and exact ray-tracing outperformed the standard formulae.


The right tools for post refractive patients
IOL calculation in post refractive patients is one of the most demanding tasks in cataract surgery. To support the surgeon with this challenge, EyeSuite IOL features a comprehensive set of cutting-edge formulas for post refractive patients with or without clinical history.
Best in class formulae for premium results
IOL power calculation in patients with prior RK, LASIK or PRK, presenting with no history, is easily achieved with the integrated Barrett True-K and Shammas No-History method. If the change in refraction caused by the refractive procedure is known, then the Barrett True-K with history, Masket and modified Masket formulae may also be used.

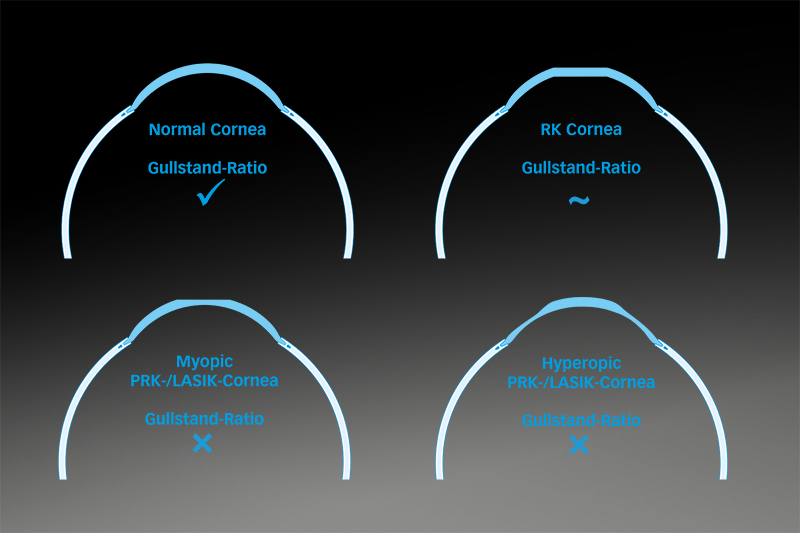
The challenge with post refractive corneas is that the Gullstrand ratio of the anterior to the posterior corneal curvature is no longer given. This leads to two main issues. Firstly, the K-readings are reported too flat with the cornea after an intervention to correct myopia and too steep for a prior hyperopic patient. Secondly, in standard calculation formulae, the lens position is calculated based on AL and K-readings. Since the Ks no longer represent the initial cornea, the lens position calculation is wrong as well. Post-refractive formulae overcome both issues by correcting either the formula or the result for the issues mentioned.

Match axis and cylinder
Getting the cylinder value and axis location right is key with toric IOL. The optional EyeSuite IOL Toric Planner features the Barrett Toric Calculator for excellent IOL prediction and an intuitive graphical planning interface to create sketches to transfer the plan to surgery.
Excellent calculation, intuitive planning
The EyeSuite IOL Toric Planner provides the user with an intuitive tool to plan the toric intervention on high resolution eye images. Using the incision optimization tool enables the surgeon to put his incision in the exact right location to achieve the minimum anticipated residual astigmatism, with the lowest toric power IOL implanted.
